
Before diving in to degenerative knee and six considerations, here’s a quick anatomy lesson: The knee joint is made of the kneecap (patella), tibia (shin bone), and femur (upper leg). On the inside of the knee joint, there exists a thick layer of connective tissue called the meniscus. The meniscus has two parts, a lateral (outside) portion and a medial (inside) portion. The meniscus is there to provide stability within the knee. Think of the meniscus as the brake pads on a car. Lastly, on the ends of both bones, “articular” cartilage exists to lubricate the joint and reduce friction as it moves. See the picture below for an illustration.
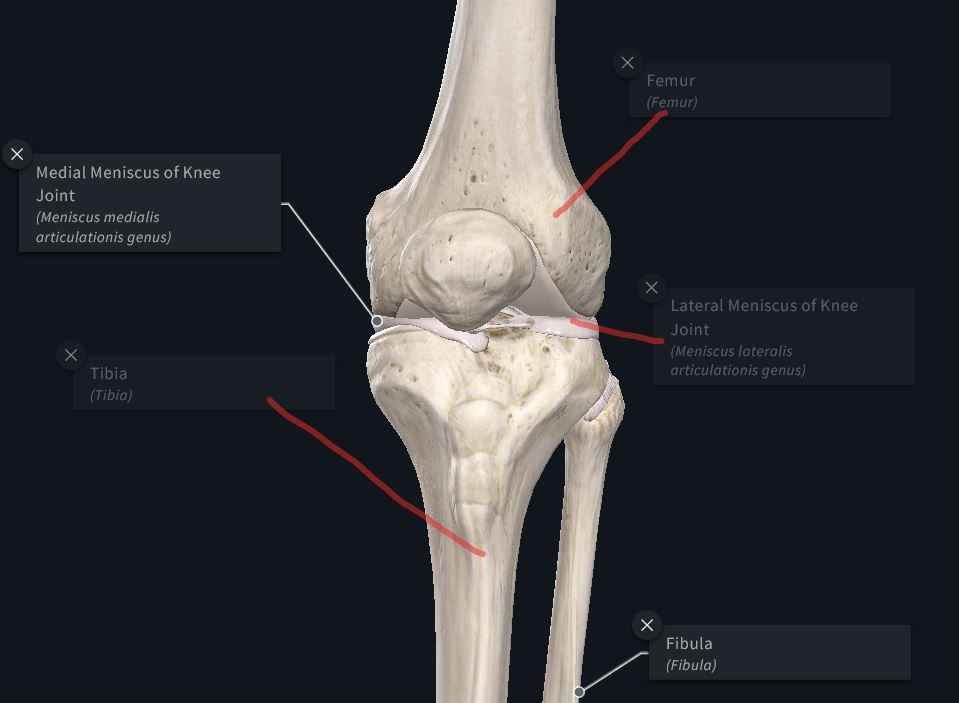
Picture courtesy of 3D4Medical.com and their Complete Anatomy App.
A “degenerative” knee is a broad term that refers to osteoarthritis (OA) or just arthritis. OA is a chronic inflammatory process that degrades the meniscus and causes pain and swelling with movement. In OA, because of previous damage, the body tells the brain to release a cascade of damaging chemicals to the area in an effort to “reset” an injured body part. The brain (usually correctly) interprets this as painful. Due to the constant signaling of damage, the cycle continuously repeats itself. OA is extremely common in people like Gurley with a history of intra-articular injuries (think ACL tear). Read more about OA here.
With this information in mind, I give you 6 orthopedic considerations when drafting Gurley.
1: Don’t let scary terms scare you away completely
A study in 2006 took 205 individuals with OA and asked them to rate their pain from 1-10. MRI’s of their knee were then compared against that pain report.
They found that “Abnormal” finding like cysts, swelling, and bone deformities correlated very poorly with subjective pain reports. In other words, a person who reports almost no pain in their daily life could have the gnarliest looking knee and never know it. The opposite is also true. Several different studies in subsequent years have validated this.
Simply put, the perception of a “degenerative knee” is overblown, and what matters are the reports from the patient, in this case, Gurley.
This leads perfectly into what does matter.
2: Watch his day to day reports
OA can be extremely unpredictable, especially when adding in several mini car crashes every Sunday. Even people who are not elite athletes report having “good days” and “bad days” when dealing with OA. Expect nothing different for Gurley. Fortunately for him, he has access to the rehab team all year around. Keep an eye on the injury report every day and every week in perpetuity to monitor his progress.
Note: The rest of this article takes you through the several ranges of outcome for Gurley.
3: Expect headaches
Ultimately, Gurley is a player to avoid early in drafts because of the wide range of outcomes that the chronicity of his condition inherently brings. This is because OA can be triggered by anything from slamming the joint into the ground to sleeping in an awkward position. Expect a weekly dance with the injury report a la Julio Jones (minus the availability that Jones usually provides).
The worst-case scenario is that in week 2 Gurley slams his knee into a 300lb linemen’s helmet triggering a 16 weeklong inflammatory nightmare and leaving the game after getting you 3 points.
Another worst-case is that his reports are bad all week, you sit him, and he goes off for 98 rushing yards, 6 catches, 40 receiving yards, and a touchdown, so you end up on the IR yourself after punching the wall.
This is the exact reason why I would not draft Gurley as my RB1 or RB2. Ideally, he’s an RB3 or flex.
4. Availability does not preclude performance
There are also several indirect factors that exist. For example, his in-game usage was so high last year, that he had no choice but to stay in peak aerobic condition. This year the active rest days could take away from that. Another indirect consequence of OA is reduced confidence. Being afraid to plow over a defender or plant hard on a jump-cut could reduce his effectiveness. These are tape grinding takes that I usually don’t ascribe to, but make no mistake, it matters for Gurley.
Which leads to consideration 6:
5. Pain is not Gurley’s only limiting factor
Fancy term alert: Arthrogenic inhibition. If you’re interested, read about it here. This simply means that when the knee takes on even minimal swelling, the brain shuts down use of the muscles surrounding the joint, usually the quads. No amount of “toughing it out” can turn this evolutionary mechanism off. In fact, the more that he tries to fight it, the worse it could become. Think of this as mother nature’s way of forcing him to rest. Gurley could have minimal pain and still not perform to his potential.
6. Gurley could be a homerun
The best-case scenario is that the Rams manage Gurley’s work volume perfectly, his body responds well to the daily prehab/rehab, and his clinical signs and symptoms are kept at a minimum allowing for a top 10 RB finish.
In this scenario, you slide him into your flex, and he goes off for 98 rush yards, 6 catches, 40 receiving yards, and a touchdown, so you celebrate by punching the wall and still end up on the IR yourself
To summarize
From an injury perspective, I am drafting Gurley strictly as a flex/RB3 (which means that in most leagues, I won’t have much Todd Gurley). If you happen to take him, keep this summary in mind.
Thank you for reading. Please make sure to follow me on Twitter @FFStudentdoc for more injury analysis.
